JeffB
-
Posts
1,086 -
Joined
-
Last visited
-
Days Won
6
Everything posted by JeffB
-
I met a gentlemen on a Celebrity cruise - I think it was aboard Summit - that actually "lived" on that ship. At the time he'd been "living there" for close to a year. The way he did it was to book inside cabins b2b2b..... at the going fare never booking more than a block of 3 at a time. IOW, you won't expereince that price increase as you get outside of 30d or so trying to book it all at once. Do it in segments. No single booking was longer than 10n (Southern Caribbean) most were 7n itineraries that Summit was doing out of PR. So, the longest individual booking was 24n. after the first 14d or so, he'd go to Future Cruises and book the next three legs and on and on and on. The ship did get chartered or went into a repair cycle over the time he was aboard. He had an apartment in Boston and he'd stay there for the short time he couldn't book his always low demand inside cabins. He was always glad to get back aboard. He was elderly when we met him. Hope he will still be at it when the lockout ends. Perhaps on another ship. I think that sort of thing is entirely doable. Just need an escape plan when the unexpected cancellation or non-availability happens. BTW, he was Zenith on Celebrity with something like 109 cruises a lot of them credited before Celebrity changed their Captain's Club rewards.
-
I flew EA6Bs from the deck of the Midway on the regular from October of 1978 to sometime in 1998. Our quarters were a bit better than those you posed but not by much. We (2 of us 03s) were forward and the cat track ran right next to my bunk.
-
State of Florida Sues CDC Over Cruise Shut Down
JeffB replied to UNCFanatik's topic in Royal Caribbean News and Rumors
This is a fair point. The mRNA vaccines in particular are very new. Traditional vaccines like the AstraZeneca and Johnson and Johnson products use a monkey adenovirus as a vector to challenge the human immune system to produce a response to SARS2. The technology is the same as that used for the vaccines you mention. Remember that efficacy and effectiveness are two different metrics used to evaluate a vaccine, the later - the real world "effect" as measured by the products ability to prevent, in these cases, serious illness and/or death from COVID. While all of the FDA approved vaccines for use in the US are in the 90% or higher efficacy range from large scale trials, that's translating to an 80% plus effectiveness in real world studies. The influenza vaccines are 30-50% effective. 97% effectiveness achieved by the MMR combined vaccines, well established by their long history of use, is unique. Don't lose sight of these numbers: in 100 cases of exposure to SARS2, regardless of risk, nominally only 5 vaccinated persons will develop COVID symptoms and of that five, less than 1 will die. Of 100 unvaccinated, at risk persons (over 65) exposure to SARS2 will produce 20 seriously ill people and of those 5 will die. IOW, unvaccinated at risk people experience a 4X greater risk of serious illness from SARS2 infection and a 5X higher risk of dying. People that are not at risk for serious illness or death from COVID become naïve hosts that will become infected, most unknowingly, and harbor the virus potentially spreading it to at risk unvaccinated people. In large scale trials monitored and approved by the FDA the rate of serious side effects or death from vaccination were as near to zero as is mathematically possible. It is true we don't yet know what side effects may occur after several years of COVID vaccines being administered. However, after about two years including trials there is nothing to suggest that the mRNA products will produce them. The adenovirus vectored vaccines have produced the blood clot thing albeit causality has not definitively been established. Moreover, the actual risk of this happening to you is almost non-existent. So, getting the vaccines comes down to a very personal and individual risk/benefit analysis. I simply want as many people as possible that post and read here to know that the risks of untoward vaccine side effects are very low while the preventative benefits when it comes to preventing COVID related serious illness or death from occurring after an exposure to SARS2 are quite high. Vaccines are becoming universally available for adults over 16/18 and some doctors offices have them. Ask if your primary care physician has them and if he does, schedule a consultation to discuss the risks and benefits. Even if he doesn't have them, visit with him or her and discuss. -
Well, yes and this negative Nancy messaging needs to stop. The example I gave of the CDC's announcement on reinfections properly condenses to the message that you have a 1 in 11000 chance of getting COVID once vaccinated. This is a hugely important one. It gets missed by the CDC and I think that is reflective of what's wrong there.
-
uhhhhh, I know where that picture came from. I highly doubt that is a picture of current cruise ship crew quarters. Maybe the SS France. The web page where this picture is on display is here: https://bestlifeonline.com/cruise-ship-facts/ More modern cruise ship's crew quarters look like this:

-
Yes. Let me be clear. The science favors multi-layered protocols for risk reduction. One of them is to require circulating virus be controlled in the locale from which a cruise ship is boarding passengers and crew then sailing. The metric by which this is assured varies but Singapore, for example, the last I checked has no deaths and no circulating virus as evidenced by new cases. There are other layers that have been discussed here. Requiring vaccinations is one the cruise industry has adopted when sailing into or from ports that aren't like Singapore or Haifa or Taipei, e.g., Nassau, St. Martin and other Caribbean ports. Why aren't we sailing from US ports yet? Well, the CDC's unworkable CSO and foot dragging is one of them. Another, however, and one that public health officials worried about SRAS2 transmission should consider before getting behind cruise ship operations from their ports, is the level of circulating virus present in and around them. Broward County, home of Port Everglades, and Miami-Dade County, home of the port of Miami, both have evidence of circulating virus (% positivity 6-8%. Generally accepted to be adequate virus control is demonstrated when new case % positivity is below 5% for 7 consecutive days). Now, given that reality, would you rather sail on a cruise ship out of either of those ports where everyone is vaccinated as an alternative risk reduction measure to insuring there is no circulating virus in both counties? In the US and globally, we will continue to see low levels of circulating virus for the foreseeable future. It might be close to 5% or approaching it but if it isn't there does that mean we shouldn't travel there? I know how I'd answer both these questions. Here's another tid-bit. Just last week the CDC produced a report that appeared on their web site that trumpeted new government data showing that 5,800 fully vaccinated Americans had contracted COVID. That may sound like a big number, but it indicates that a vaccinated person’s chances of getting COVID are about one in 11,000. The chances of a getting a version any worse than a common cold are even more remote. But what trumpeting news like that does do is to discourage vaccination - exactly what the Biden administration is working hard to avoid. Vaccines are the best alternative that will allow a return to normalcy as a means of approaching and then achieving herd immunity in the US. A fully vaccinated boat-load of crew and passengers HAS herd immunity and an exceedingly small risk of anyone aboard becoming re-infected either aboard or ashore in a port of call or getting seriously ill from COVID even lower risk. Here's a link to a cool model based on available data sets. The interactive graphs at the link are titled "A Path to Normality." The US approaches the stage when all mitigation measures can or should be removed in May and achieves it in June. https://covid19-projections.com/path-to-herd-immunity/
-
Let's be clear. The WHO is an organization with deep roots in policy recommendations and guidance that place equity and justice at the forefront. I'm not advancing the notion that is a bad thing. In some cases it is completely appropriate and under-recognized. TBF, developing policy that is both pragmatic and at the same time advances equity and justice is a very tough job. Here's the key statement in the linked document: Do not require proof of vaccination as a condition of entry, given the limited (although growing) evidence about the performance of vaccines in reducing transmission and the persistent inequity in the global vaccine distribution. States Parties are strongly encouraged to acknowledge the potential for requirements of proof of vaccination to deepen inequities and promote differential freedom of movement. Earlier in the document, the WHO acknowledges the impact of vaccines in reducing COVID related deaths and illness as well as reducing the Transmission of SARS2. They correctly call for relying on the emerging science. They go on to say there's not enough evidence yet to definitively conclude that vaccines are as good as they seem to be. What? This is the problem with the WHO. The last statement in the quoted text demonstrates that deepening inequities and differential freedom of movement are more important than improving global public health. IMO, it is blindingly obvious that requiring vaccines for entrée to specific venues (e.g., large gatherings to watch sports, airline travel, sailing aboard cruise ships) will decrease both disease burden and transmission. Don't require these because it is unfair? The Israeli's have it right ...... "you will be left behind if you don't get vaccinated." That is being pragmatic. The WHO isn't being pragmatic.
-
There are a dwindling number of those politicians I believe. I base that on the bills that members of Congress are submitting - maybe it's good theater but a lot of work goes into submitting a bill. Members know or are told by senior leadership if a bill has no chance of even being considered. Don't submit it. We'll there are 2 bills submitted and probably another that will be. I think Congress, unattached to the current executive, would come to the same conclusion about the NSO, CSO and the crippling of the cruise industry as we have. It's unwarranted and probably not lawful - that's another story by itself winding its way through the courts. The more I write about this, the more I reason it out, the harder it gets to see anything remotely sensible about it. People packed in at the beach, at an airshow, OUTSIDE? The risk of spreading the virus is as close to zero as it gets. Not only has that risk been overplayed, it simply is unscientific to keep showing pictures of crowded outside venues to imply they are potentially super-spreader events to sew virus fear and should be banned.
-
I'm sure that the flurry of activity directed at the CDC's over-reach over the last two weeks isn't changing anything. I gave it two weeks from the Desantis filing to see if the needle moved. Not a bit. The non-sensical advisory from the CDC that endangered citizens of St. Vincent, should not board a cruise ship sent to the island to either transport those citizens to safety or provide safe food and water is beyond monumentally stupid. It demonstrates exactly where the CDC is on the cruise industry and on it's COVID narrative that it's advancing. They are unable to or refuse to do an appropriate risk/benefit analysis. This sort of analysis seems to be completely missing in the Biden administration's approach to the pandemic. That's very disappointing and I think it characterizes the likelihood that we are going to see any substantive changes to the current circumstance that is crippling the cruise industry. We know that MSC has essentially abandoned the US and Canadian cruise market for this summer to restart on a larger scale in Europe. They're getting the jump, and wisely so, on the rest of the industry. I think RCG is hopeful that some kind of rapprochement is possible with the CDC and I'm sure they've run the numbers. But, my take is that if the CDC continues to take the position they have apparently taken, the rest of the majors will leave the US market this summer for whatever is available in Europe. That is going to be hugely damaging to the service sector that supports cruse ship operations ..... I just don't get this. Failing to recognize these costs with minimum COVID risks to re-starting accompanied by benefits that clearly out weigh those risks is mind-boggling to me. But, I'm preaching to the choir. And to Europe.....at one point I had foreseen European ports opening to cruise ships before US or Canadian ports. I felt that in February the EU had the virus contained and vaccines would guarantee its further retreat. Hasn't happened, except in the UK. The more noteworthy circumstance, however, is that Spain, Greece and Italy, some black sea ports, probably Israel and some other mid-eastern ports will open to cruise ships because their economies are highly dependent on tourism. That's a plus but, still, for US and Canadian citizens, you have to get there. Air travel will require lots of hoop jumping, the added expense of air-fare and uncertainty over cross boarder travel within Europe.
-
Honestly, the CDC has simply lost all credibility with me. I'm absolutely convinced that it is the best interests of the CDC and the Biden administration to continue the negative messaging that characterizes most of what they are putting out there these days. It is intended to change human behavior in the face of SARS2. It's not working. I'm watching rather gleefully that facts on the ground, the US economy, the declining disease burden as measured by hospitalizations and deaths, what appears to be a county by county decline in % positivity commensurate with the level of vaccine roll-outs - there are exceptions but as has been predicted these are regional and reflective of a shift from a pandemic to an epidemic (regions) - states removing mitigation measures and more and more people going about their daily lives. All of this and more belies the CDC's (and the Biden administration's) negative narrative augmented by the media.. Admittedly the US economy is booming due to Fed stimulus. I consider this good. Most should. The bottom line is that the CDC and it's faces, Walenski and Fauci, appear to be becoming irrelevant. Some one needs to get in Joe Biden's ear. He could become a hero by changing the administrations tone ...... get vaccinated and things will improve as quickly as we can make them improve and that depends on you getting vaccinated. He could signal that change by canceling the NSO and CSO and using the cruise lines as shining examples of how to layer mitigation measures, including the requirement to get vaccinated if you want to board one of their ships, making them THE singular safest place to be to gather with friends
-
Thought I'd post some interesting and good news today. We need that. Read an interesting Bloomberg News piece on government's authority to mandate vaccines. A good deal of it dealt with Governor Desants' EO banning "vaccine passports." His intent was to ban such requirements for a patron to enter any business operating in FL under a FL business license. There was lots of misinformation about this pretty narrowly focused EO as you'd expect that implied it had broad effect and would include cruise lines. I had argued it won't as I understood it. The debate continues - mostly because controversy is newsworthy. Let's clear some things up: A requirement to show proof of vaccine for entry wouldn't violate HIPA as has been claimed. That is because the entity requiring such information isn't a healthcare entity. According to the lawyer quoted in the Bloomberg piece, "there is no statutory, regulatory or constitutional bar to that (a requirement to show proof of vaccination for entry) to happen as long as it is applied in a non-discriminatory manner." I think that last legal opinion is definitive on it's face. Clearly that's not going to end the debate. What I think is clear is that the cruise lines have looked at the legal implications of requiring vaccinations to board and have decided that it is necessary layer of many other mitigation measures and requiring it is legal. Plan on getting vaccinated if you want to board a cruise ship when cruising restarts. I like that Desantis was quoted as apparently implying the cruise industry would be required to comply with his ban. I can't find that direct quote. I also think that given his strong support for the restart of cruising, if he actually did say that, there are plenty of ways for him to side-step it. In other vaccine news is you haven't heard it already, Pfizer has announced "a third shot (a booster) will likely be required 12 months from the date of your second shot." I never thought there was any question that SRAS2 would become seasonal much like influenza and that annual shots would be recommended to blunt it's effects. SARS2 is with us. I think this is good news. It indicates Pfizer thinks SARS2 will become seasonal and immunity will wane over time. It will need to be boosted. Like the influenza virus, its genomic makeup will vary. The one thing we have going for us is that these mRNA vaccines have 90-90% efficacy with effectiveness, even in the face of variants, around 80% effective in preventing death, serious illness and transmission. Flu vaccines are between 35 and 50% effective. A CBS's 60 Minutes segment aired on Sunday. It featured a scientist who works within DARPA (The Defense Advanced Research Projects Agency) who described two pretty amazing advancements that "would stop the next pandemic in its tracks." (Link belwo) The reason I mention this is that most of us are suffering from pandemic fatigue and have lost some hope for the future. We'll let me tell you scientists and researchers haven't lost hope and continue to advance technologies and therapeutics in ways unimaginable a decade ago. https://www.cbsnews.com/news/last-pandemic-science-military-60-minutes-2021-04-11/ Unrelated to COVID, my daughter is such a researcher. She lives and works in Switzerland. Her work involves supervising a research project that builds synthetically derived tissues that when assembled become an organ. One can then test the effect of a therapeutic without involving human trials. The net result is speeding the introduction of advanced therapeutics through the regulatory process. A kidney and liver have already been assembled. Proof of concept is underway. Have nice day! ?
-
........I should add that the legislation just submitted that by law established by Congress would lift the CSO is a nice gesture. First it has to get out of committee and I'm not well enough informed or inclined to understand the whole process. Would welcome additional insight on this process and the chance a bill could go into affect in the next 30-45d. I don't think it is possible so, just more theater I would think. The law suit filed by FL has a chance to move the needle but the State's Attorney office doesn't seem to be knocking on the door of the judge that will hear the case. There is such a thing as an expeditious or emergency hearing. The state is mum on that. My hope for that suit having an impact is fading. I gave it two weeks. There are two days left.
-
Possibility? Sure. Actually happening? I remain skeptical. The Biden administration's pandemic policy is overly cautious to the extent bad policy is developed. e.g. the FDA recommendation to pause J&J vaccines that became policy by approval. Costs exceed any benefit, IMO. Moreover, messaging remains confusing, often contradictory and hard to flesh out purpose and intent of it. Despite enormous pressure to lift the CSO from various quarters, the CDC needle hasn't moved. If anything we're seeing retrenchment, foot dragging and digging in of heels.
-
Will I need COVID vaccine booster shots before my cruise?
JeffB replied to PG Cruiser's topic in Royal Caribbean Discussion
First, the vaccine manufacturers may or may not be involved in the studies that are designed to assess the long term effectiveness of their vaccine products. Second, we do not yet know with any kind of certainty what the biomarkers are that are called correlates. These are one or a set of many serum biomarkers that correlate with immunity to reinfection over time. Correlates are determined by corelate analysis studies. These studies are done in government labs within agencies like the National Institute of Allergy and Infectious Diseases in the US among others. University labs also do these kinds of studies with grants from the feds. The effort is global in nature. Some small studies have looked at B Cells (noted above), and others, in post vaccinated subjects to predict the length of time immunity to reinfections persists. So far, so good: https://science.sciencemag.org/content/371/6529/eabf4063 One of the great things that happened during the pandemic is the tremendous global cooperation between researchers and scientists whose specialty areas are infectious disease. I know that the question of how long immunity will last is on the top of the list of things to identify for public health officials. The human immune system is incredibly complex and a lot of how it works remains unknown. We know that there are lab tests (titers) that can detect specific and known elements of the human immune system that give us an idea of estimated levels of immunity for a particular virus .We know, for example, what those are for Mumps, Measles and Rubella (MMR), among others, by doing titers, but it usually takes a decade or more to ID them and plan re-immunization protocols to restore lost immunity. But a correlates analysis has to be undertaken, is an ongoing process, with certainty regarding which biomarkers are reliable in identifying continuing immunity from SARS2 infections emerging over time. This is a complicated way of saying we still don't know how long immunity from SARS2 infection lasts and won't know for a while. So far, we know reinfection after SARS2 vaccination is rare with only a few known cases out of millions of vaccinated people since vaccines became available to the public just less than 6 months ago. Large scale trials began at least 9 months ago so those subjects can be looked at too. So, we can conclude, anecdotally, that immunity lasts at least for around 9 months. This shouldn't surprise anyone but from the little I know about virology, SARS2 is going to be a seasonal virus that will require re-vaccination. Is it every year, every 3 years? 10? We will know that better once solid correlate analysis points to reliable biomarkers whose presences in human serum can identify immunity, I also suspect that as a result of the damage this pandemic did, public health officials will be quick to recommend revaccinations every 12-24 months by the time January 2022 rolls around. -
Is there nothing more conflicting in cruising than...
JeffB replied to smokeybandit's topic in Royal Caribbean Discussion
........ balancing what's actually happening on the ground with SARS2 and COVID and what politicians, public health authorities and the media seem to want to tell us is happening. -
I get the point of your post but I'm perplexed as to why you feel "insulted" by Fain's remarks. He's never said, nor implied that the July 4th is the planned re-start day for RCL cruises. I believe you inferred that. What he has said is this: "My fondest desire is that we can follow President Biden's target of July 4th as a major reopening milestone. The evidence is that we can do it. Now is our opportunity to work together towards that common goal." That last sentence is an important rejoinder suggesting RCG isn't doing any sailing from US ports until the CDC either lifts the NSO/CSO in it's entirety or revises the CSO. He's said, along with CLIA, he thinks the CSO is unworkable and lacks identifiable gates and a time line for reopening. IMO, he, along with CLIA, are spot on You won't find a more informed group of cruise fanatics who post here regularly and probably do read everything and anything having to do with the restart of cruising. You're the first to post that you are "insulted" on the basis that you believe Fain thinks that cruise fans are not informed. There are some issues. I've posted that I have become frustrated by RCL's lack of forthrightness. Same for the cruise industry titans in general for their lack of courage and leadership ...... that was before the flurry of events I spoke of above a little more than a week ago. That was leadership from CLIA, from all the cruise line CEOs that chimed in challenging the unfairness of the on going situation and Governor Desantis making that very claim in a law suit filed in the federal district court system of the State of FL. I've stated on this message board that I'm waiting patiently to see what comes of the flurry of events that culminated in FL's Governor Desantis announcement on Friday, April 2nd, that the State of FL was suing the Biden administration over the closure of FL ports to the cruise ship industry. Will the needle move? So far, it hasn't budged. I'm frustrated but, I'm certainly not insulted by anyone in the cruise industry who is dealing with the incredibly difficult leadership and management requirements of their positions.
-
Will I need COVID vaccine booster shots before my cruise?
JeffB replied to PG Cruiser's topic in Royal Caribbean Discussion
This is a good question. Matt has already provided an answer. Here's what's behind that answer and what you are probably hearing from health care providers and public health officials. The 6 month thing is based on data available since the introduction of vaccines both in trials and to the public. That goes back about 6 months, no further ..... yet. After 6 months, Trial data from the four principal vaccines - Pfizer/Bio-N-Tech, Moderna, Astrazeneca, J&J - all of them large scale involving thousands of adult subjects, demonstrates that antibodies to SARS2 were present after 6 months. Emphasis on SARS2 because there are now three principal variants that have been shown to have reduced effectiveness against transmission. None of them have shown reduced effectiveness in reducing deaths. They're all doing fine in that regard and only slightly less effective in reducing serious illness. Those are the facts and none of this came from the press where you will read all sorts of misinformation about variants. As we learn more about how effective the vaccines are against emerging variants, boosters may or may not be required. Scientists and vaccine manufacturers are already working on this. mRNA vaccines (Pfizer and Moderna) are reportedly very easy to modify as genomic variants appear so, if we need boosters, these will be what we'll probably get regardless of what we initially received. Keep in mind, efficacy and effectiveness are not the same. Trials demonstrate efficacy and all three of the principal vaccines have around 90% or better. Measuring the effectiveness of a vaccine involves seeing how it actually works in the real world over time. Some data is available from the trials and effectiveness is a bit lower than efficacy but still the vaccines work and work very well in preventing serious illness and reducing transmission. So far this has been true for all three of the variants recognized as being more transmissible but not more deadly. https://www.gavi.org/vaccineswork/what-difference-between-efficacy-and-effectiveness?gclid=Cj0KCQjw38-DBhDpARIsADJ3kjl_2zMSPDBjlMj4chOc68hc9YL6aX1ZU5h9X569ElWU4zoeRwFwCNQaAgouEALw_wcB -
There's mounting evidence from Michigan, among other states, that teens and kids are becoming infected with the more transmissible UK variant at fairly high rates. Fleshing out the actual numbers and comparing them to a baseline in the under 20 age group though is hard. I've accessed several data bases and what is being said by Governor Whitmer in MI and echoed by Dr. Walenski of the CDC isn't precisely born out in the data I'm looking at. Youth sports, for example, is being touted by Governor Whitmer as a prime source of viral spread and increased new cases in MI. But, from a baseline, it's not under 18s - I would suppose that's who participates in youth sports programs - that this increase is being seen. It is predominantly in the 20-39 yo group. So????? I've become very skeptical of COVID related pronouncements coming from politicians and the CDC. The issue for cruise lines and kids is not one of increasing disease burden in this age cohort (hospitalizations and deaths), it is one of the risks of undetectable viral loads in early infections that get missed by molecular (PCR) or antigen testing as part of a pre-boarding health screening process and then asymptomatic transmission aboard ship as the infection progresses. It's also one of the lines evaluating the risks versus the benefits obtained of allowing families with kids under 18 to sail in the current environment. My take is that allowing under 18s to sail without vaccination (or 16s if you want to include soon to be available Pfizer vaccines) and with only a negative PCR test to board, does increase the risk of a shipboard COVID outbreak but probably only among other kids who boarded. It's still an outbreak, it should be a medical concern worthy of trying to avoid even though it's not likely to be one that produces serious illnesses. I also believe that the risk of transmission from an infected kid to a vaccinated older adult is very low. However, on any re-start scenario approved by the CDC and within the next few months the best strategy is to not take that risk of allowing kids to sail. So, if I were providing input to the Healthy Sail Panel that involves decisions about sailing in the current circumstance, I'd say vaccines should be required for al. passengers. At some point, COVID will be a manageable infectious disease similar to influenza, norovirus or the common cold. Kids can sail then. That point gets moved up as kids and everyone else gets vaccinated. But until either of those points are obtained, I'd advice against unvaccinated persons being allowed to board regardless of a pre-boarding negative test result.
-
Things are really getting serious now....
JeffB replied to dodgestang's topic in Royal Caribbean Discussion
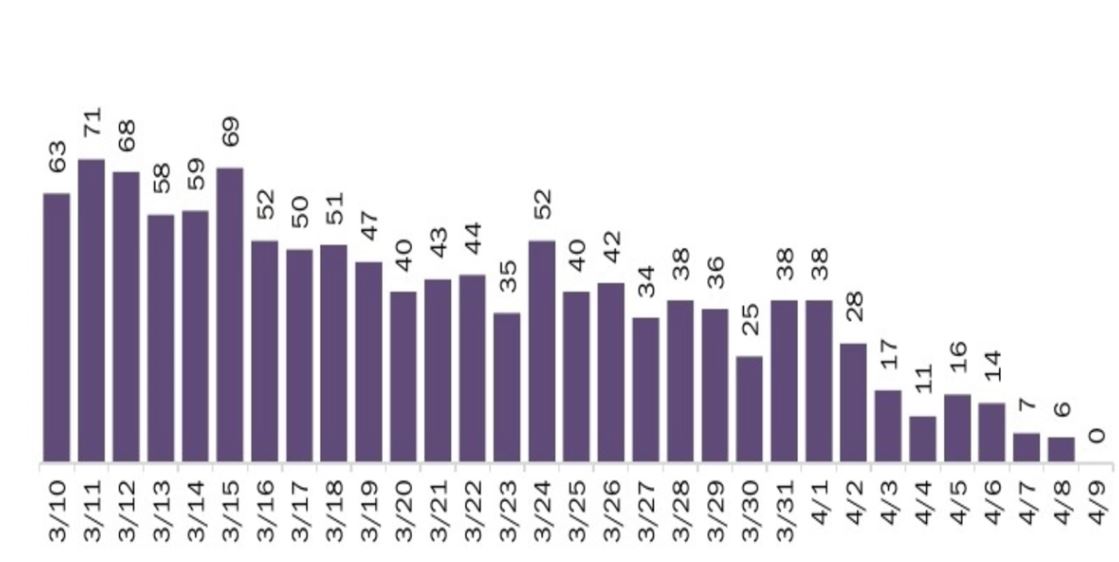
I mentioned yesterday that the impact of COVID is likely less than we are led to believe it is. A lot of this has to do with how public health officials report COVD data and then how the press presents it to us. Giving us case numbers out of context is misleading. For example, on 3/9, FL reported 5007 new cases. A month later, on 4/9, 6817. That's a 36% increase in new cases yet the percent positivity over that same period went up only 1%. When you test more, more new cases are identified...... testing on 3/9 = 175/100K. Testing on 4/9 = 282/100K. That's a 37% increase in daily testing producing an expected 36% rise in new cases. On 3/9, FL had 3419 patients hospitalized with a COVID diagnosis. On 4/9, 3016. But this is the kicker - deaths: Need I say more? Florida is fine.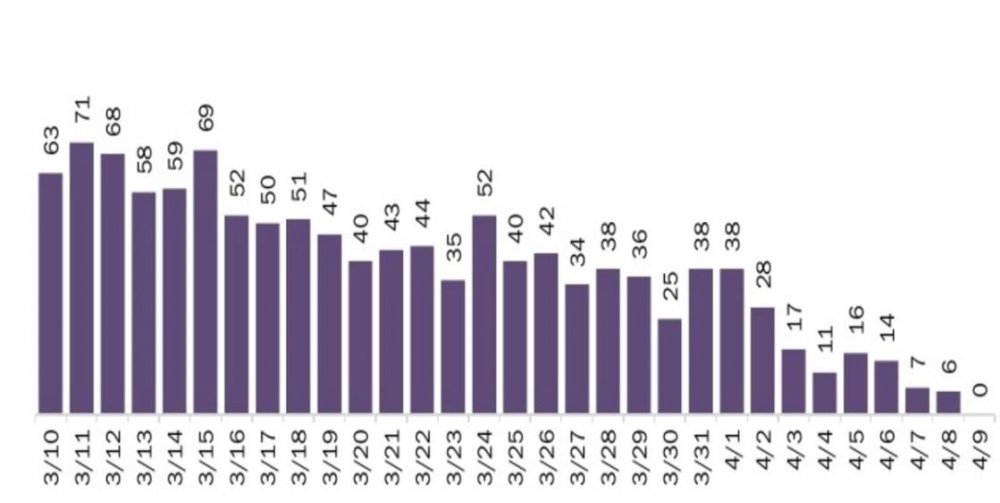
-
Things are really getting serious now....
JeffB replied to dodgestang's topic in Royal Caribbean Discussion
Well, yes, but only directly in one small segment of activities in the US impacted by the CDC's "the boogey man is coming" messaging. The SARS2 pandemic is a problem. No denying it. But I remain shocked that the word's governments response to it, after a year of dealing with it, fails to recognize that it is a problem that has to be dealt with by means other than scaring people and having those governments encourage regional entities (the states and counties) to issue more and more restrictions to mobility and/or restrictions to business activities. One thing I believe is that the impact of the COVID is far less than we are being led to believe it is, that, given the advancements in COVID treatments and the effectiveness of reasonable mitigation measures make it so ..... and I've never believed this whole thing is a hoax. It's real. It's a real problem but it is one that can be overcome with a combination of vaccines, through increased testing, effective identification and targeting of regional outbreaks for specific and time limited mitigation measures and an effort to restore confidence in US public health policy making entities, namely the CDC. That last one is important because I believe what's happening in the US now - the increased violence and discontent - is largely a result of this "boogey man is coming" messaging emanating from the CDC, augmented by the press that loves a crisis. Instead of that, I'm advocating for a change in tone from one of worry to one of confidence that the virus can be brought to heel. Start with defining a path forward to the resumption of a reasonable post-pandemic normalcy and that includes revisions of the CDC's CSO. -
Things are really getting serious now....
JeffB replied to dodgestang's topic in Royal Caribbean Discussion
Just one of the problems the cruise lines are dealing with in getting sailings restarted from US ports is the wrongheaded focus on COVID case numbers as an indicator of pandemic status by public health officials, the CDC being the worst offender because they know better. This gets augmented by the press as they love a crisis. Then the public mood and by extension, public health policy is shaped. Because of the distorted view of where we really are with controlling the transmission of SARS2 and the disease burden of COVID it's impossible to define a path forward to post-pandemic normalcy. For us cruise fanatics, we see this glaring problem reflected in the NSO, the CSO and the lack of a clear path forward to the resumption of cruising from US ports. There are better metrics than COVID case numbers to measure the impact of the disease. Not only that but the impact of COVID is highly regional. The disease burden in MI is different than it is Kansas yet the CDC uses one figure - new case numbers - applied nationally to cast every state in the same dire situation. I think Desantis, among other governors of similar persuasion, mostly has the right idea. I'd look to the UK's Boris Johnson though who has pursued an aggressive and prioritized vaccination strategy, similar to Desantis, et. al., but has combined this with highly targeted restrictions on citizen mobility based on a testing strategy that is unique in the world. The UK is doing more testing, particularly genomic testing, to guide the targeting of regional hot spots for mitigation measures. That is smart. They also have a robust national contact tracking and tracing program. The results, so far, are striking. We'll see if it continues. Sadly, we are stuck with the Biden administration's CDC. I don't see them changing their messaging or outlining a pathway back to a post-pandemic normalcy. Sticking with the CSO, it appears, is reflective of that lack of COVID insight and vision so badly needed here in the US. While there is talk of more testing and the addition of the genomic type, I don't see guidelines from the federal level that trickle down to well designed public health programs at the state level. Ostensibly, that could help guide emerging and improved public health policy on a state by state basis that is more focused and targeted. I just don't see it happening and I don't think vaccines, alone, are going to sufficiently change new case numbers enough to change the public mood and by extension, public health policy. Sadly. The pending law suit by the state of FL might have an impact if only in the context of our interests in a return to cruising. Despite how good I think the plaintiff's arguments are, I still think it's a long shot. What we need is a wholesale change in how leading experts from the CDC view the impact of SARS2 going forward while outlining a responsible return to a post pandemic normalcy. If FL wins the case and gets an injunction, that could move the CDC to re-evaluate more than just their approach to the cruise industry. Mid to long term, that's what we need. -
State of Florida Sues CDC Over Cruise Shut Down
JeffB replied to UNCFanatik's topic in Royal Caribbean News and Rumors
I've been under the impression that the only businesses affected by the Desantis position on vaccines are those operating in FL under a FL business license. I don't think that whatever the cruise lines decide is going to be their vaccination policies would be affected by the Desantis position. To my knowledge they're not required to obtain a FL business license and that they don't have one is why retail shops onboard close when ships are in port. Not sure how bars are affected because they are serving in port. There's another complicating matter. Ports in FL operate in certain situations under federal jurisdiction. The NSO springs from that. The feds mandated masks in those facilities that come under federal jurisdiction, e.g. airports, train stations, etc. I suspect some port operations are impacted by federal laws. We already know the feds aren't going to mandate vaccines. So there appears to be no conflict between federal law and the Desantis vaccine position. -
State of Florida Sues CDC Over Cruise Shut Down
JeffB replied to UNCFanatik's topic in Royal Caribbean News and Rumors
So what happens next? The case will be put on the court's docket. I don't see that an emergency hearing was requested. It might be at a later date if it appears that the case won't be heard fast enough for the lawyers arguing the case. There will be a preliminary hearing. The judge's clerks will have prepared briefs in advance for him that he will have read. Both sides will present arguments for and against. The judge can rule or he can postpone pending additional information. The Justice Department lawyers defending the CDC will request that right out of the box. The plaintiff's attorneys will argue time is of the essence and I believe that argument has legs. We'll get to watch the Justice Department lawyers try to defend the laugher that is the CSO. Hate to be them! The plaintiff will seek an immediate injunction based on the arguments presented to the judge. The case seems strong to me but, I'm a lay person. The law is quirky and a unsuccessful outcome for the plaintiff is usually due to stuff that people untrained in the law find hard to understand Let's say the judge rules. He can either grant the injunction the plaintiff seeks, deny it or order some other undertaking (e.g., why don't you guys sit down and work this out with an arbitrator). The $64,000 question is what if the judge grants an immediate injunction? Well, the cruise lines have from whenever in April to the end of June to get a limited and carefully selected number of ships and crews ready to accept passengers; ports have the same amount of time to rehire workers and train them. July cruises will sail. From what ports to where and on what itineraries will emerge over the next few weeks. Exciting times. -
State of Florida Sues CDC Over Cruise Shut Down
JeffB replied to UNCFanatik's topic in Royal Caribbean News and Rumors
IMO, this is a slam dunk case. Yet, OJ was ruled not guilty. I don't think there is any question that the court has jurisdiction and the case has standing in the Middle District Federal Court (Tampa). The government will try to have the case dismissed claiming everything that has been done by HHS and the CDC is authorized under the PHE declaration. In reading the case file, I can see that FL lawyers already have anticipated that and addressed it in the counts below. I don't see any technical obstacles. The counts are effectively described with appropriate case law sited Count 1: Agency action not in accordance with law and in excess of authority. The suit alleges that the CDC was granted authority under US Code (USC) to do specific things. It goes on to allege that the CDC both broke the laws granting said authority and exceeded it's authority - mainly and in this case, by locking down the cruise industry through November, 2021. The suit alleges it has no authority to do that. Count 2: Arbitrary and capricious agency action. ......a court must “hold unlawful and set aside agency action” that is “arbitrary [or] capricious,” as Defendants’ actions are here. Argument is made that multiple other and similar businesses are open or are reopening with appropriate and reasonable mitigation measures and are operating safely. Only the cruise industry's business activities have been unlawfully restrained. Count 3: Agency Action Unlawfully Withheld or Unreasonably Delayed. In the alternative, and for the same reasons stated in Count 2, Defendants’ failure to allow the cruise industry to safely reopen constitutes final agency action unlawfully withheld or unreasonably delayed, in violation of 5 U.S.C. § 706 Count 4: Failure to Provide Notice and Comment. This one is complicated but nonetheless strong. Basically it alleges that the CDC sought public comment, got it and did nothing with it. We weren't privy to this but I'm sure the cruise industry people working with the CDC complained about this and will now get their day in court. Count 5: Unconstitutional Exercise of Legislative Power. A straight forward legal argument. Quoted here: 71. Article I, Section 1 of the U.S. Constitution states, “[a]ll legislative powers herein granted shall be vested in a Congress of the United States.” Under Article I, Section 1, only Congress may engage in lawmaking. 72. If the Conditional Sailing Order does not exceed the authority under 42 U.S.C. § 264 and the relevant regulations, then Section 264 constitutes an unconstitutional exercise of lawmaking by the executive branch, affording the CDC the power to determine the rights of millions of citizens, to decide on the survival of countless businesses, and to make a host of sweeping policy decisions absent meaningful accountability. Kind of a back-up, catch the CDC if the Judge rules for the defendant on the other counts. Finally, what is the state of Florida asking for. Again a quote because it is clear and succinct just like the Judge wants them to be: PRAYER FOR RELIEF For these reasons, Florida asks the Court to: a) Hold unlawful and set aside the Conditional Sailing Order. b) Issue preliminary and permanent injunctive relief enjoining Defendants from enforcing the Conditional Sailing Order. c) Postpone the effective date of the Conditional Sailing Order. d) Declare unlawful the Conditional Sailing Order. e) Declare that the cruise industry may open with reasonable safety protocols. f) Award Florida costs and reasonable attorney’s fees. g) Award such other relief as the Court deems equitable and just. -
State of Florida Sues CDC Over Cruise Shut Down
JeffB replied to UNCFanatik's topic in Royal Caribbean News and Rumors
This The case was filed today in Federal Court. Current listings for the Middle District only go through the 7th, but I'll find it tomorrow. Until I can read the entire case filing I can only speculate about the details so, here's that speculation: The case isn't likely to be a tort claim although one of the criteria for such a claim is damages. So, there is that - the cruise industry can show that in terms of lost revenue. Tort claims are intended to fully restore a plaintiff and the cruise industry isn't asking for money. They want to sail and will seek a court decision where the judge enjoins enforcement of the NSO. This is more likely to fall into the category of an Administrative Procedures Act/Review or Appeal of Agency Decision. I had suggested elsewhere that the easiest target in obtaining an injunction might be a violation of 14A - to wit: undue restraint of trade or commerce. The Plaintiff, in this case the state of FL, would seek to have the judge declare the CDC's NSO and by extension the CSO an unconstitutional restraint of trade and therefore unenforceable by DHS. Things get tricky with the PHE declaration by HHS. That is both constitutional and lawful as far as I can tell and the NSO and CSO derive from that. Attorneys for the Plaintiff would have to argue that while the PHE grants the CDC authority to restrict activity that presents a public health risk (e.g., cruise ship operations and every other economic endeavor associate with those), such restrictions of the cruise ship industry's operations run afoul of 14A (undue government restriction of trade and commerce). This was not the case in March 2020. The risk of disease spread was unknown but presumed to be high in congregate settings. Made sense. At this point, the risks of SARS-2 transmission are more fully understood and we have layered mitigation measures designed to reduce such risks. These have been developed and proven to be successful in preventing C-19 outbreaks within the travel and leisure sector of the global economy. Yet the CDC says cruise ships, unlike other similar travel and leisure venues that are operating now can't operate from US ports? I don't think that is defensible. Vaccines are the game changing wild card. When the Plaintiff throws that card on the table as a means of reducing the risk of transmission aboard a cruise ship to near zero by itself and then add in the other layers of protection the cruise lines have adopted, I'd like to see Justice Department lawyers defend the overly complex and burdensome provisions, required only of cruise shops while not of similar travel and leisure venues of the CSO. Anyway, I'm not a lawyer so TIFWIW. I had fun speculating. Gives me hope that the CDC clown show is going to get pantsed in court of law.