JeffB
-
Posts
1,074 -
Joined
-
Last visited
-
Days Won
6
Everything posted by JeffB
-
Close call (Covid) on Adventure with happy ending!
JeffB replied to Jill's topic in Royal Caribbean News and Rumors
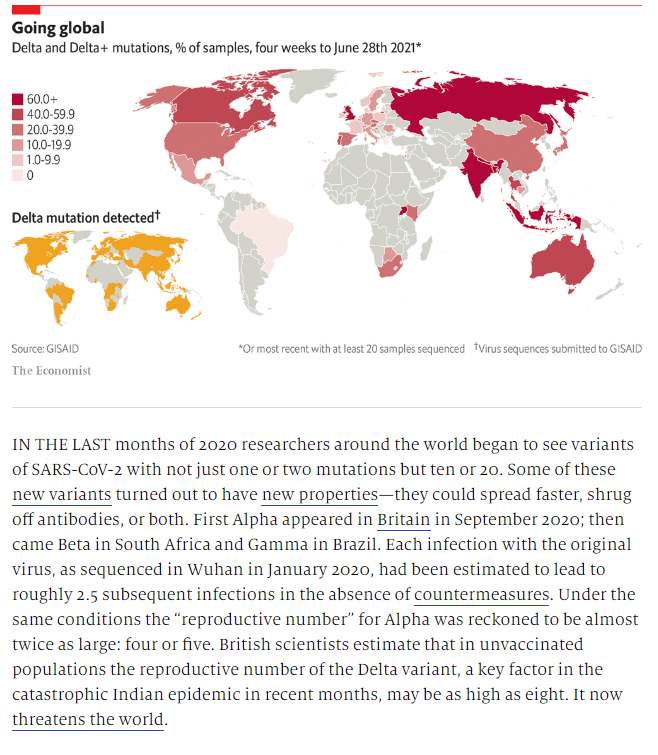
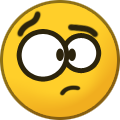
Good stuff @LizzyBee23 thanks for posting that. I'm not an alarmist by any measure but the increased transmissibility of the Deltas is a real factor in prolonging this thing. I see this circumstance as a bogey that is imminent and should be dealt with appropriately. I still don't think we should or will see major and widespread restrictions to mobility and business activity but there will be inconvenient re-imposition of mitgation measures in places where vax rates are low or risks of transmission high..... indoors in congregate setting. It is not too hard to see the potential for SARS2 obtaining greater capacity to evade our immune systems, vaccines and therapies when it is left to percolate globally. See below:
-
DeSantis/Florida wins prelim injunction over CDC
JeffB replied to smokeybandit's topic in Royal Caribbean News and Rumors
I am also uncertain but I think that if Desanits had not advanced legislation to make his EO - which was issued under authority granted to him in the state's PHE - the EO ban on asking for prrof of vaccination would have also expired. But it's now law in the state of FL. It could be challenged but it would be an uphill road to do that. -
DeSantis/Florida wins prelim injunction over CDC
JeffB replied to smokeybandit's topic in Royal Caribbean News and Rumors
I just noticed this today and it really doesn't bear on FL V. Bacerra but there's no other good place to put it. Governor Desantis let Florida's PH Emergency declaration expire last Saturday. The only thing I saw in the news is that his failure to extend it will eliminate compensation/reimbursement for telemedicine. Apparently, the FL legislature will submit a bill to extend the financing for that "in the next session" whenever that is. I suppose it isn't starling news and not in the category of "if it bleeds, it leads" journalism. OTH, if I have this right, there is a ton of stuff tied to it and the expiration of the PH emergency pulls the rug out from a lot of it. For example, let's say that Miami-Dade county discovers a cluster of COVID within cramped living quarters for migrant farm workers. The county PH agency is going to be restricted as to what mitigation measures they have at their disposal to do anything about it. The PH emergency was fundamental to giving the counties authority to do something like that. Of course, although I don't know the details, when Desantis made the move a couple of weeks ago to forgive any COVID related fines or charges along with him previously saying the counties can't do anything that restricts mobility, closes businesses, requires masks, none of that stuff is authorized any longer. Same for schools that are doing summer school right now or summer camps. So, letting the declaration of a PH emergency expire last weekend may be a nothing burger from a standpoint of how residents and businesses might be affected. But when financing for COVID related projects, funded by the state or the feds, gets cut off there's an impact. I could see the same for health and safety protocols already put in place for summer school and camps - we'll see what it is, I guess. Some journalist will pick up on a "catastrophe" related to this and pin it on Desantis. -
Close call (Covid) on Adventure with happy ending!
JeffB replied to Jill's topic in Royal Caribbean News and Rumors
I agree with the thrust here @LizzyBee23. The current level of hysteria about the variants in the US, especially given the high vax rates among vulnerable populations is unnecessary. In countries with high vax rates, we should be thinking endemic pathogen of interest and managing clusters of it discreetly. I think this is what you mean. One thing to keep in mind is that while COVID is a URI, the possible outcomes from contracting it, unlike a URI or Flu, are significant across select age and medical status cohorts. You do make the point that each cruise ship has to be equipped to care for COVID cases that go south and to quickly off-load passengers whose clinical status depends on a level of care not available on the ship. I don't know the details of the capability to do that across the RCL fleet. Can they intubate and ventilate on board? Administer anti-cytotoxic therapies, Administer antibody treatment? These are all life saving early interventions and then the question becomes, as you say, what happens if there are 15-20 cases, 10 of them are over 65 and at risk and 5 of them are already starting to go down hill with low O2 Sat levels. I have a gut feeling the medical staff has the same kinds of protocols for dealing with a very ill COVID case that looks a lot like how they treat an MI or CVA case (Advanced Cardiac Life Support, Stroke Prootcol - both complicated with specific drug and imaging requirements.) So, I'm not ready to say, "treat COVID like any other URI. What I am ready to say is that you manage a shipboard COVID positive, unlike a URI, very aggressively with isolation of the positive(s), aggressive contract tracing and quarantine (note isolation and quarantine are different animals) until a diagnosis is confirmed or rejected by a molecular test (PCR and others - and I don't know for sure what RCL is using among molecular tests. It should be RT-PCR as this test is the most reliable diagnostic test but it also requires special and specific handling and processing in a Clinical Laboratory Improvement Amendments (CLIA) certified lab. That's a big deal. Failing to aggressively manage a shipboard positive case just presents so many possible untoward outcomes that it just isn't worth the risk of less aggressive approaches and I don't think you're suggesting that. A no-kidding outbreak involving an older cohort could quickly overwhelm the ship's medical facility. A death aboard a cruise ship, during transport or immediately after admission to a hospital's COVID wing would quickly end cruising. -
Your points are taken, @smokeybandit I read the article. I was unaware of Prasad whose made a name for himself pummeling the CDC. Nevertheless his 5 failures section of the article is a worthwhile read in forming perspective and listening to both sides. There is no question that how the CDC presents its data and how others do is subject to legitimate debate. Despite this, I think the predominant messaging from the scientific and medical community is that the risks of COVID among unvaccinated children is higher than the risk of myocarditis in that cohort. that is a nation wide perspective and I think regionality is missed as @Jkaczanonotes. There are those that disagree with the CDC's recommendations. Prasad is one of them. I practiced medicine as a PA for 22 years. One thing I learned: Doctors don't agree on much. One can parse the data and Vinay Prasad does a lot of this in an effort to disparage the CDC's position on vaccinating kids ..... it's like piling on. They've made errors. It's easy. Walenski, whenever she opens her mouth, usually inserts her foot. As I've held all along the CDC is terrible at messaging. I read a short Twitter exchange between Vinjay and Rochelle. He's merciless. OTH, the CDC collects the data and does a pretty good job of doing that and interpreting it. Others might disagree and that is understandable in science and among researchers that are looking at this emerging PH threat. Like I said, nothing in science is certain until it is absolutely proven so and that rarely happens.
-
Thank you for your response @Jkaczano New Hampshire has been recognized as a leading state in managing the SARS2 pandemic. The low seroprevalence does mitigate toward the rationality of your viewpoint on vaccinating your children. I've always held that COVID and it's impact is regional and generalizations that consider the entire US can, themselves, be misleading. Having said that, the level of regional transmission in your state is still considered high (see the link below). So, to me, that would seem to mitigate toward vaccinating them. This statement, also at the link, seems to indicate a low occurrence rate of myocarditis such that, as the chart I posted above shows, the risks of Myocarditis from the mRNA vaccines are exceedingly low while the risk of COVID infections inthe cohort we are talking about is still fairly high: There was not a safety signal identified at time of last VaST report (May 17th): reports of myocarditis after COVID-19 vaccination did not differ from expected baseline rates – Multiple causes of myocarditis, including: viral infections (cold viruses, COVID-19), bacterial infections (Lyme disease), etc. https://www.dhhs.nh.gov/dphs/cdcs/covid19/documents/hcp-call-presentation-052721.pdf I respect your position though vis-vis your children not getting vaccinated. Just keep an open mind and be convincible.
-
At the request of @cruisinghawgI'll reluctantly respond to this and a few other comments: Not really ........American Citizens have no Constitutional protection from being told by a state vaccinations are required. Nearly 100 years ago, the U.S. Supreme Court issued its landmark ruling in Jacobson v. Massachusetts,33 upholding the right of states to compel vaccination. The Court held that a health regulation requiring smallpox vaccination was a reasonable exercise of the state’s police power that did not violate the liberty rights of individuals under the Fourteenth Amendment to the U.S. Constitution. The police power is the authority reserved to the states by the Constitution and embraces “such reasonable regulations established directly by legislative enactment as will protect the public health and the public safety” (197 U.S. at 25, 25 S.Ct. at 361). It is good to understand the history of how the requirement for vaccinations emerged in the US. I's all right here: https://www.cdc.gov/vaccines/imz-managers/guides-pubs/downloads/vacc_mandates_chptr13.pdf Look, I get the concern about children being vaccinated and putting thier safety above any sense of duty to the public health. This is true especially given the short history of the COVID vaccines approved in the US. One needs to be on point when they take that position. In a that was then, this is now sort of dialogue, distrust of the state has increased dramatically since Jacobsen v. Massachusetts. But the FDA has remained as apolitical and balanced as any government agency in this pandemic - the rigorous testing protocols that pharma has to comply with in brining a drug to market, even under EUA, and with the exhaustive review process the FDA conducts, all the US approved vaccines are very safe. Yet misinformation about their effectiveness and safety flood social media platforms as in, "that decision (not to vaccinate a child) is a no brainer." It is? Really, based on, "Right now, with cases averaging 22 per day on a population of 1.4 million and multiple cases of myocarditis locally." I doubt both the validity of the numbers and how these are being presented. These are the facts: CDC numbers through late May estimated that 16 cases of myocarditis or pericarditis would be reported for every million second doses given to people ages 16 to 39. That works out to 0.0016%, or roughly 1 in 62,000. By contrast, de Lemos said the best studies on college athletes put the chances of a young person getting myocarditis after COVID-19 at between 1% and 3%. That's roughly 1 in 50. https://www.heart.org/en/news/2021/06/21/should-rare-cases-of-heart-inflammation-put-your-covid-19-vaccine-plans-on-hold There's more: Though fewer children contract COVID-19, and fewer kids and young adults experience serious illness, there’s still some risk of contracting the virus. Since the beginning of the pandemic, at least 7.7 million COVID-19 cases have been reported among people ages 12 to 29. In May, that age group represented 33% of COVID-19 cases. Since the beginning of the pandemic, 2,767 coronavirus deaths have been reported among this age gr https://whyy.org/articles/myocarditis-and-the-covid-19-vaccine-what-to-know-about-rare-heart-inflammation/ And then there is this: All of the foregoing facts seem to indicate that it is a no-brainer to not get your kids vaccinated. Profiteering by big pharma as an underlying cause of distrust of vaccines is also a frequently held parental concern. IMO, that denigrates the work of 100s of dedicated scientists that worked on these vaccines and deployed them in record time. I don't think that circumstance is fully understood by critics of big pharma. That pharma developed these in a public private enterprise is perfectly good reason for these companies to be rewarded and the public to benefit from the miracle drug the mRNA vaccines are. I reject that concern as largely baseless. Now of course you could argue that the Chinese and the Russians who deployed Sinovac and Sputnik through government nationalized production did just fine. But they didn't and countries that received these vaccines in a form of vaccine diplomacy are battling reinfections. https://www.nytimes.com/2021/06/22/business/economy/china-vaccines-covid-outbreak.html One final comment on another set of stats that are floating around on social media platforms that vaccine nay-sayers grab on to without checking them out. The conflations and missuses of absolute and relative risk along with vaccine efficacy abound in social media platforms then trickle down to casual conversations. The link will take you to a great article that describes these misuses, how believable they appear and how utterly dangerous they are to rational, well informed thought on getting vaccinated or not. https://www.reuters.com/article/factcheck-thelancet-riskreduction/fact-check-why-relative-risk-reduction-not-absolute-risk-reduction-is-most-often-used-in-calculating-vaccine-efficacy-idUSL2N2NK1XA All of this sounds like lecturing and badgering those who aren't vaccinated or don't want their kids vaccinated. I apologize for that because it is the least effective way to change people's minds on any number of COVID and Pandemic related views and especially in the hotly debated arena of vaccinations. Generally it's hard to do. But judgements based on inaccurate or misleading information are dangerous. What I encourage is not blindly rejecting or accepting, even being moved by what I've posted here but rather keeping an open mind to views contrary to your own. Become convincible. Join legitimate focus groups led by doctors and scientists. Ask questions.
-
On a whim? (1) we're talking about a public health crisis involving a pandemic that has caused the death of 1/2M people in the US. There are medical therapies that can be used to subdue it's impact that include vaccines. (2) There are laws that allow businesses to fulfil their moral and ethical responsibility to create a save environment to do business. Taken together I can argue we have a civic duty as Americans to follow the law and be ethically and morally responsible. YMMV, JMO, I am heavily biased as a medical professional toward vaccination ....... I am also stepping over the lines that Matt has established for discussions like this. I'll read but that's the last of my post on this thread on vaccinations, whether or not they work and whether or not those able ought to get them. that's reared its head again and I'm guilty.
-
Its an unpopular position to articulate support for the CDC. Their public messaging hasn't been good. They have themselves to blame for that. However it is the politicians and the press that "politicize" their recommendations and public statements that come from the CDC. I'm not a fan of Anthony Fauci either and the reasons for that go beyond his credentials as a virologist - those are solid. He is always very careful - hedging is the operative term - not to get pinned down. Listeners don't like that but he's a scientis and few things are certain in science, especially emerging science on SRAS2 and COVID. The CDC, in most circumstances that do not involve regulatory authority (I'll get to that), provide recommendations for PH matters. They don't direct anything and since the mask debacle in February 2020 and the Trump administration telling CDC folks to go sit in the back of the room and shut-up, CDC spokespersons have been very careful to make that clear. The most recent clarifying statements wrt that involve the position they took on masking when their recommendations (no masks for vax'ed) differed from the WHO's recommendations (masks indoors regardless of vax status....... Walenski's response when asked about this (paraphrased) "we are recommending no masks for the vaccinated in the US but leave decisions in that regard to local PH authorities." I think the CDC is spot on regarding no mask wearing required for vaccinated people in the US. I'm pretty sure you would not disagree with that. The CDC does, in fact, have regulatory authority over the cruise lines through the Vessel Sanitation Program (VSP). The authority I am most familiar with is what is granted under 42 U.S.C, Section 264. Regulations pertaining to preventing the interstate spread of communicable diseases are contained in 21 CFR parts 1240 and 1250 and 42 CFR part 70. https://www.law.cornell.edu/cfr/text/42/71.1 When Merryday ruled in FL v. Bacerra, he did not say the CDC doesn't have regulatory authority. They do. What he said is that aspects of the CDC specifically directed at the cruise industry were, for all-intent-and-purpose, new laws that the CDC does not have the power to write. Most of the legal arguments presented by FL's attorneys revolved around the limited time frame that free pratique can be denied via the VSP. That argument carried the day and the details of why it did, including pages of citing case law going back hundreds of years is in his written ruling. The link below describes the CDC's regulatory authority for the cruise line. https://www.cdc.gov/nceh/vsp/default.htm I can't agree with this generalized statement. There is some uncertainty about responses to vaccines v. natural immunity with certain T-Cell types. With others there is no uncertainty - for example, CD4 and CD8 T-Cells showed a marked decrease following infection with SARS2 that are not seen with vaccines. In fact, the T-Cell response with the mRNA vaccines is robust (confounding factors in several studies were not isolated. The article linked below pertains. https://www.news-medical.net/health/What-are-T-Cells.aspx WARNING: we can easily both get in over our heads in this area. What I try hard to do within this forum when I post about COVID is to eliminate my biases or admit them and not make generalized statements that may not be supported by the facts. Nevertheless, in social media platform like this is authoritative statements frequently become gospel when the statements conform with a particular readers biases and preconceived beliefs. It's not easy to remove biases from posts. Admission of a bias and links to facts supporting a viewpoint are helpful. I really have a problem with sweeping generalizations intended to support a POV.
-
Immunity from SARS2 is immensely complex. My review of the literature on this subject indicates that there is plenty of disagreement among research scientists about how much and how long immunity is conferred by a previous infection. Fundamentally, your body has two types of immunity: humeral and adaptive. You've all read about B Cells. A previous SARS2 infection resulting in even mild cases of COVID trigger a humeral, B Cell response. Your bone marrow produces these. Exposure to SARS2 also produces an adaptive T-Cell response. In both cases, it is not yet known with any certainty how effective your immune system will be in protecting you against reinfection if you've had COVID in the past or how long that immunity might last. It is also not conclusively known that any of the currently US FDA approved vaccines will produce better or worse protection against COVID. Research trends suggest that vaccines produce a more robust and complete immune response (humeral and adaptive) v. COVID than natural immunity from a previous infection. Research trends also suggest that people who have had COVID benefit from a further increase in immune response to SARS2 by getting vaccinated. I am knee deep in the controversy over vaccination. I still believe in choice but as the pandemic plays out it is getting harder and harder for opponents of vaccination, those who are eligible and able, for any number of reasons, to justify that position. The CDC, even though they have made missteps, is still a solid collector and interpreter of available data. Sure, they've lost the trust of many of us. I am not among those mainly because I follow the research literature on this closely. But, I'd call the position that the CDC has taken, opposite to that of the WHO on masks is solid and is better reflective of the SARS2 transmission situation in the US. The WHO has a more global perspective and where viral transmission is at high levels, it is generally believed masking helps reduce it ........ all the controversial aspects of human behavior and other factors that bear on how masks are worn, how effective they are, not withstanding. As far as the cruise lines are concerned @AshleyDillois correct. They are not going to allow those who have been previously infected by SARS2 with proof of antibodies be considered immune. Frankly, I don't think anyone should consider themselves immune from infection by SARS2 if one has had COVID. I would add that the current crop of AB tests have flaws - and there are a lot of them , including home tests that you can buy over the counter. Cruise line health and safety experts are also going to go with the most conservative approaches to all COIVD related practices.
-
Key West Voters Approve Ban on Large Cruise Ships
JeffB replied to SpeedNoodles's topic in Royal Caribbean News and Rumors
I read several of the briefs that were submitted to journalists by the primary supporters of the large cruise ship ban from Key West. Not one of them provided any solid science that the Key West reefs, surrounding waters or environment were threatened by large cruise ships. It was all voodoo science foisted on the Key West public who then thought, yeah, this is bad, ban them! The port and local businesses didn't really get involved until it was too late (their fault). Of course the ban supporters have accused Desantis of paying back a Key West developer who has money in the port for a large contribution he made to the Desantis campaign. Fine. I don't care. That common sense prevailed over a bunch of environmental loonies is good for Key West and good for the state. There is always compromise paths to walk that take inot account the needs of both interests but environmental extremists are a tough lot to deal with and tend to drag along followers who really don't understand what they are getting into. JMO. That's not to say that Cruise lines don't need to be conscious of FL's environmental issues in the barrier reefs and that entire eco-system. I have no doubt that they do care and aren't willing to run afoul of the various regulations, enforced by the USCG designed to portect these sensitive areas. Seaman are a very conscientious lot when it comes to the oceans - of course the garbage and sewage dumping of a miniscule portion of maritime operators get the news. For every 1000 sailings, there may be one that breaks discharge laws. They get caught and suffer large fines. -
DeSantis/Florida wins prelim injunction over CDC
JeffB replied to smokeybandit's topic in Royal Caribbean News and Rumors
Based on what we're seeing with both test cruises and 95%'ers that are being operated in full compliance with the CSO, whatever the CDC comes up with is going to be changes in the language of the current CSO to make it legal under the CDC's authority granted in 42 U.S.C. Section 264 Quarantine and Inspection Regulations to Control Communicable Disease. At the onset of this thing I was skeptical that FL would prevail. As the arguments unfolded it became more apparent that they would and Merryday's ruling was pretty clear. CDC overreached among other things. If Merryday feels that a good faith effort is made by the CDC to adjust some of the language. He could simply vacate the injunction. Iwould hope in any rewrite they do that they are consulting with the cruise lines on some of the more onerous requirements of the CSO like test cruises and volumes of reports and legal standards for contracts. While it's true that after the CDC does its work and submits it to Merryday, there's a period of mediation to follow. There are two outcomes: (1) FL agrees to the changes and there is a settlement, (2) FL does not agree and it goes back to Merryday like last time. I don't think Merryday wants to force a rewrite of decades of complex maritime law by enjoining the CSO and essentially sending an open ended set of unenforceable regulations back to Congress for a rewrite of parts of U.S.C. 42, Section 264. I have a gut feeling he will rule in favor of the CDC providing the CDC in it's rewrite meets Merryday's expectations. That might seem to leave FL out in the cold. That's how the cookie crumbles. He might throw them some crumbs. What that might be is uncertain. -
Points Guy article re: Celebrity Edge today
JeffB replied to Jill's topic in Royal Caribbean News and Rumors
Lots of stuff at play. If I'm reading the charts above correctly, they end in December 2020. Certainly, vaccines are going to dampen surges. I think most experts agree that there might be a rise in cases come fall and winter but disagree on the extent of it with vaccines in the mix of causal factors. The percentage causality of the many factors coming this fall is going to be hard to sort out. If you go to the home page of Hope-Simpson modeling (link below) there's lot to be learned from the graphs and charts. The link hopefully will take you to a side by side comparisons of the US, UK (both with high vaccination rates approaching 70%) compared to Norway (low vaccination rates around 42% and in the far northern hemisphere). The difference in new case numbers are similar both in terms of absolute numbers and trends. If a rise in case numbers we are seeing in low vax rate US states have "noting to do with Delta's (or variants in general) and more to do with cold weather associated with seasonal changes, you would expect to see new cases increasing in the colder Norway. They aren't. If the link goes to the home page you can either bleive me or use the various toggle to set up the comparison above. You took issue with my statement that, "The thing about the Deltas worth bringing up is that in states with low vax rates, hospitalization rates have started moving up for the first time in 2 months." To which you responded, "This has nothing to do with Delta, but with the seasonal viral effect in lower latitude states." The CDC thinks there is a correlation between the increase in a US state's new case number, seroprevalence of the Deltas and vaccination rates absent seasonal viral effect in the lower latitudes. Many aren't listening to anything the CDC has to say and I understand that but in this case the likelihood that they are interpreting the available data correctly in the US is pretty high. Part of my point in the original post was that as vaccination rates per region/country/locale/ increase cruises will trend toward increasing normalcy. The higher the vax rate on each ship, the better. That vaccines are dampening new case numbers in high vaccination rate places absent temperature variants is going to help a return to cruise normalcy. Every reasonable metric of disease burden points to the conclusion that vaccines work. It's hard for anyone to deny that and I don't think you are doing that. http://hsmap.rice.edu/map/gds -
Points Guy article re: Celebrity Edge today
JeffB replied to Jill's topic in Royal Caribbean News and Rumors
Sure, that's contributing but not alone. Here's an expert's take on seasonality: Challenges Seasonality of COVID-19 Hardy doesn't agree with the IHME's experts that SARS-CoV-2 is seasonal. Last winter's surge, he noted, occurred to a much greater extent on the West Coast and in the Midwest than in the Northeast, where a seasonal trend would have been expected because of the cold weather driving people indoors. This is a decent article that looks at causality and experts disagree on causality of COVID surges. Certainly seasonality is a player wrt increased COVID cases but there are other factors too (human behavior, transmissibibility of variants, vaccination rates etc.). I think the CDC does a pretty good job of assigning causality to a rise in new cases. To me and in the current time frame, I believe vax rates are playing a significant role in the rise in case numbers. My post focuses on vaccination rates but there are other factors as you point out. https://www.webmd.com/lung/news/20210520/what-experts-predict-from-covid-this-fall-and-winter -
Points Guy article re: Celebrity Edge today
JeffB replied to Jill's topic in Royal Caribbean News and Rumors
Good stuff @JasonOasis In reading the morning news, there's a small piece on the Edge sailing - first cruise ship sailing from a US port since March 2020. Great. The most "important" news was worry about Delta and now Delta + variants. Of course it had a political part to it. You'll know what it is so no need to bring it up here. The thing about the Deltas worth bringing up is that in states with low vax rates, hospitalization rates have started moving up for the first time in 2 months. This is worth fleshing out if you are interested. I've gotten adroit at finding the kernels of truth at the CDC web site among the mountains of data residing there - it's hard and it is why journalists have trouble putting the Deltas in perspective. So you can make sense of the graphs at the second link, the Delta variant is B.1.167. The link takes you to the chart of the SE region. You can select any region you want on that page. https://www.cdc.gov/coronavirus/2019-ncov/variants/variant-info.html https://covid.cdc.gov/covid-data-tracker/#variant-proportions My take aways: The Deltas are not a threat to people who have been vaccinated. (The US overall is very close to 70% vaxed) As of right now, there is an almost imperceptible but nevertheless real up tick in what I call "disease burden" as measured by ED visits for COVID like symptoms and hospitalizations. You have to look regionally to see these. It is not wide spread in the US. Upticks in these metrics are closely associated with vaccination rates, i.e., the un-vaccinated are the ones going to the EDs to seek care and/or getting hospitalized. There is notable shift to younger aged cohorts and that is because those cohorts also correlate with low vaccination rates both by circumstance or choice. It appears to me that PH focus on the Deltas, here and abroad, as a means to push people to get vaccinated will complicate political decisions to re-open Lets look at this statement in light of the above: Generalizing that question to one that asks when will things move closer to normal aboard cruise ships operating in a world of COVID? Not any time soon is my response. Experts augmented by the media continue to warn that "the pandemic is not over." IMO, that's overkill. It has certainly been subdued but mainly in countries that are hitting vax rates above 50%. Country COVID circumstances and regs will continue to drive cruise line's safety and health protocols for at least another 18-24 months and this will apply especially to sailing to or from foreign ports. For example, even though sailings from non-FL ports are operating with 95% or above vaxed pax manifests, in Greece, because the Greek government still imposes an indoor mask mandate, cruise ships operating from there require guests onboard to be masked indoors (usual exceptions apply). Caribbean and Alaska sailings are the ones most likely to more quickly move closer to normal ops. That is because US, including Hawaii, and Caribbean ports are even now enjoying low viral prevalence rates and that should improve over time. EU sailings will lag, but only slightly, behind US cruise activity. Same for Canada but slower still. Asia sailings are going to be tough and that will impact transpac ans pacific Island cruising. By country low vax rates are hurting these regions. I can't even speculate how quickly this situation will improve. Things are too fluid. South American sailings? Probably even tougher. Don't count on improvement in that cruising region for a long time and if there's a restart, the voyages will be highly restricted. Australia and NZ? Man, who knows? Those governments are locked into lock downs to quell outbreaks. It kinda makes sense on Island nations but that tendency will continue to have a significant impact on cruising in that region. None of this is particularly good news but I think for us cruising fans its a wake-up. The regions where we can cruise and enjoy some normalcy in the short term are limited. I'm fine with that as long as I can get back on a cruise ship somewhere. But those bucket list cruises to EU ports will start slowly and those form Asian and South Pacific ports we're probably going to have to wait a while. -
That's one way to look at. Another is to consider that Princess had an R(0) of 2.6 back in March of 2020. That means an exponential time independent increase of infections of around 3X, 9X, 81X and so forth......a very steep curve of new cases. TBF, R(0) values apply to a completely naive/unvaxed exposed cohort. Clearly vaccines have helped, so has previous infection and conferred immunity therefrom. So your view has merit. It is unlikely that going forward and as the pandemic wanes, R(0) values are going to remain closer to 1.9 and below at their peaks and we are actually seeing that in places with vaccination rates > 50% where the Delta variant is being reported as "surging." Rates of new infections are low - remember "flatten the curve"? That's what vaccines and conferred immunity from previous infection are doing. Of course those details and context are not being reported - we just get a continuing fear monkey narrative. Those of us who have supported the development and implementation at the re-start of clear protocols for the handling of COVID positive crew/pax on a cruise ship either by CSO enforceable regs or by HSP recommendations consider that an important aspect of the line's responsibilities. That extends to their responsibilities to keep guests, crew and the communities they call on as safe as possible from COVID outbreaks. That starts with immediate isolation of case #1, contact tracing and quarantine of those who meet the criteria for that and, importantly in this discussion, how and where a ship makes a port call to off-load infected persons. Beyond that are all the other shorebased steps needed to make sure there's no community spread in the port area/city the ship is off-loading infected people. Personally I don't want the cruise lines or port authorities to make shit up as they go along, neither did the CDC or, for that matter the cruise lines through the HSP as far as we can tell. While it is true that the risk of that happening on a fully vaxed sailing is very low, slightly higher on a hybrid sailing, why not be fully prepared for that even remote occurrence? We've already seen that scenario play out a couple of times. It's happened and will happen again. These protocols and agreements worked. I'm glad it was all planned out before hand.
-
.........@smokeybandit also seemed to imply that "port agreements" come in two flavors: Home Port berthing agreements and port of call agreements. If I'm not mistaken, and this may be @smokeybanditpoint, the CSO didn't make a distinction between the two, just saying (1) ports couldn't ban cruise ships from entering with COVID cases aboard and that (2) to make that workable, the cruise lines had to do X, Y & Z with regard to the handling of COVID cases being evacuated from the ship - this to prevent the Princess fiasco - and ports had to contractually agree to whatever the parties came up with on that score.
-
allure returns in 2026 All Things Galveston
JeffB replied to Galveston Steve's topic in Royal Caribbean Discussion
It would be nice to know if CCL got broadsided by an unexpected request for either the CDC or the port authority to provide an advanced pax manifest ....... or ....... if they screwed this up knowing full well they needed to give advance notice. In a close read of not a well written article on this, it's possible that pax weren't filling out health questionnaires during the before terminal arrival check-in process done on an app or at the web site correctly. If so, not their fault and from what I see among cruise people (not here because we are all well informed ?) there's plenty who don't know about and therefore don't do what they are supposed to do when doing advanced when check in for a booked reservation. -
allure returns in 2026 All Things Galveston
JeffB replied to Galveston Steve's topic in Royal Caribbean Discussion
I thought this was interesting: Carnival Sends Last-Minute Requirement for Guests on First Four Cruises First, Carnival is a line that has previously announced it is sailing under the provision of the CSO to restart without CDC monitored test sailings and instead a 95% vaccinated pax manifest. Second, I've offered that RCL "opened a can of worms" sailing with test cruises and a hybrid pax manifest. What I find interesting is that cans of worms aren't limited only to lines that want to sail with a hybrid pax manifest to protect access for families with unvaxed kids. In this case it appears Carnival is in a pickle trying to insure, in advance???, that they have vaccination proof for 95% of pax. They're asking in this unexpected email sent to booked guests to go to their booking and fill out an additional health form stating that if you don't do this, your booking may be cancelled ..... wow! ..... I suspect most guests expected to simply show their vax cards during the boarding process and, if I'm not mistaken that was the intial guidance. Now, either the company or the CDC is asking for advance proof. This could have something to do with the federal requirement to close out pax manifests 48h before sailing. https://www.cruisehive.com/carnival-sends-last-minute-requirement-for-guests-on-first-four-cruises/52473- 965 replies
-
- 1
-

-
- msc seascape
- presidents cruise
- (and 16 more)
-
Very nice monkey wrench in our cruise plans, advice?
JeffB replied to RCIfan1912's topic in Royal Caribbean Discussion
Let your TA sort it out. Your situation is somewhat unique but as @AshleyDillopoints out the CWC program allows you to cancel without penalty. If there's an upcharge for your new baby at 8 months of age, it should not be full fare. Usually, third person in cabin comes at a reduced cost. Congrats on the "bun in the oven." -
Precisely ........ this is the hallmark attitude, among others, that we need to carry as sailing resumes and our own sailings materialize. The other one is insure your risks. That doesn't just mean travel insurance. For some it's required for others, it's a good idea. Even though the cruise lines appear to be offer what amounts to full medical and evacuation coverage, you may need coverage for other medical emergencies. Know and take advantage of the cruise line's protections. Book your air through the cruise lines when it's available. That way if the sail dates change, the line will take care of re-booking - it happened to me for an October cruise out of Barcelona and air was rearranged at no cost to me. Travel insurance has gotten expensive, especially for seniors, if you are insuring against COVID or if you want "cancel for any reason." Explore plan options. I've come to the conclusion that I have primary medical coverage through my insurance plans but I'm almost positive I'd end up paying a bundle after primary coverage paid out. I don't think we know how good the cruise line's medical and evac coverage for a COVID related circumstance. So far for the two teens and their families on AoS it worked. Keep in mind that is just for a COVID related illness. That could get tricky if, for example, you tested positive for COVID but had a heart attack. Medical Evacuation is costly. When I was younger and my risk of illness was lower, that's all I bought. Things are different now so, I purchase comprehensive coverage. Try not fully insuring the cost of your trip. For example if the whole trip costs $5K, buy $3 or $4K - cost goes down the less the insured dollar value you buy is. I've not had any luck in trying to exactly match what medical coverage I have with a travel insurance plan. The coverages are fixed, e.g., $24K, $50K,, etc. So, I guesstimate and look for the lowest cost coverage with the highest reimbursement value for a medical event. I also try to buy policies with the highest medical evacuation coverage. The actual cost of having to do that from Europe or Asia, for example, can be astronomical. From the Caribbean, not as high. Good hunting.
-
New guidelines out for July sailings out of FL
JeffB replied to Lovetocruise2002's topic in Royal Caribbean News and Rumors
OK, show of hands. How many of you that are vaxed or unvaxed and booked on FoS in July will cancel because of this? My take is that it's good accommodation. The Casino lock-out might be a show stopper for some but the rest, eh. -
This is a solid take. We tend to over focus on the path to resumption of sailings from US ports as if it's a one way street to that objective. It's not. I actually think the port agreements thing in the CSO was good (without some of the enforcement provisions). OTH, I'm not sure that the cruise lines weren't pursuing more COVID robust agreements on their own (that is in the HSP). I have a Celebrity Equinox sailing booked in August that had a stop in SJ. About 3w ago, I got notified that the SJ and DR port calls were cancelled and replaced with a sea day and a call at Nassau (not great but glad to be sailing). I doubt this news will change Celebrity's operational plans even though it is 60 days out. Too many moving parts.
-
I'm not a regular FB user but Lisa Lutoff-Perlo has a FB page so I messaged her and asked if she might use her good offices with the Greek government and get them to give Apex a pass on indoor masking being that almost everyone on that ship will be vaccinated. I doubt she'll respond. Her page isn't very active. There is one sailing of Apex before the one I'm booked on. It's possible there wont be a mask mandate indoors for my cruise. The Greek SARS2 situation is improving rapidly as vaccines are finding arms. Even 2w ago, things were improving in the face of open boarders with proof of vaccination or negative COVID test required to enter.
-
Just watched Edge sail from PEV on the port's web cam. Captain Kate backed her down into the shipping channel, did a 140 and off she went. I literally got all choked up and balled my eyeballs out. Funny thing, I could have sailed on this trip if I hadn't gotten all wrapped up in thinking sailings from US ports wouldn't happen before September with the CDC's stand and the hardships of complying with the CSO requirements facing the lines. Thought Europe would be first for sailings with US citizens. Booked Reflection out of Amsterdam in February for a early June sailing to Norway - then Europe fell apart with another outbreak. Cancelled that booking and moved it to tourism friendly Greece. That one is going on July 9th but I have to fly 11h to Athens ...... and wear masks inside and outside (standard exceptions) due to Greek COVID protocols that mandate masks. Isn't Celebrity and it's weird. So, could not do both although I was sorely tempted. Burned through all my FCCs. If I hadn't I would have booked Edge for today. Anyway, it was spectacular watching that beauty leave the pier. Some stories I read today that the crew was jazzed and so were the passengers. 40% capacity. Celebrity announced they were 99% pax vaccination rate. Celebrity has the same vaccination rules as RCL but they don't attract as many families ..... obviously with that rate. I'd like to know how they got there. Edit: Just checked ....... Greece just yesterday removed max mandates ....... outdoors for now. Other restrictions on restaurant capacity and gatherings are being eased too. Still have the mask mandate indoors and I expect Celebrity will honor that unless the Greeks give them a free pass with pax and crew fully vaccinated. That would be welcome. Go Lisa! You can do it!